
A Rational Proposal in Planning and Performing the Ochsenbein-Luebke Flap in Endodontic Microsurgery
Received 26 September 2025
Revised 23 January 2026
Accepted 24 February 2026
Published online 05 March 2026
J Endod Microsurg. 2026;5: 100020.
Under a Creative Commons license
HOW TO CITE THIS ARTICLE: AMA STYLE
Tkachenko O. A rational proposal in planning and performing the Ochsenbein-Luebke flap in endodontic microsurgery. J Endod Microsurg. 2026;5:100020. https://doi.org/10.23999/j.jem.2026.5.1

ABSTRACT
The choice of incision and flap design in endodontic microsurgery is an important stage that significantly affects the success of the operation. Each flap has its own technique and indications for implementation. It is also necessary to take into account many other important factors: which tooth is being operated on, the length of the tooth root, the size of the periapical lesion, the gingival biotype, the existence of periodontal diseases, etc. It is rational to choose a flap according to the above factors but bearing in mind possible complications as well. One of the flaps that has fewer complications than others is the Ochsenbein-Luebke flap. The indications, contraindications, advantages, disadvantages, possible complications and features of the implementation of this flap were analyzed in the article. A sensible proposal for planning a submarginal flap and indications for its implementation according to the clinical situation of a patient are described.
KEYWORDS
Ochsenbein-Luebke flap, endodontic microsurgery, indications, contraindications
INTRODUCTION
Successful endodontic microsurgery requires a solid knowledge of endodontics, periodontology, and oral surgery. Therefore, the surgeon performing endodontic microsurgery must carefully consider this knowledge during treatment planning.
A flap is defined as a section of gingiva and or mucosa surgically elevated from the underlying tissues to provide visibility and access to the bone and root surface [1]. Selecting an appropriate flap design determines the success of surgery [2].
Various flap designs exist at present, but the endodontic surgeon must understand that:
-
All flap designs have both advantages and disadvantages.
-
No single flap design is amenable to all surgical cases [3].
The most popular paramarginal or submarginal flap is the one designed by Clifford Ochsenbein and Raymond G. Luebke (1974) [4, 5]. The Ochsenbein-Luebke flap is formed by a scalloped horizontal sub-marginal incision placed within the attached gingiva, which follows roughly parallel to the contour of the gingival margin. The horizontal incision continues with two vertical releasing incisions [6]. These vertical incisions extend from a point 1 to 2 mm short of entering the mucobuccal fold to a point on the attached gingiva approximately 3 to 5 mm above or below the marginal gingiva and the sulcus depth (Figs 1 and 2) [7, 8].
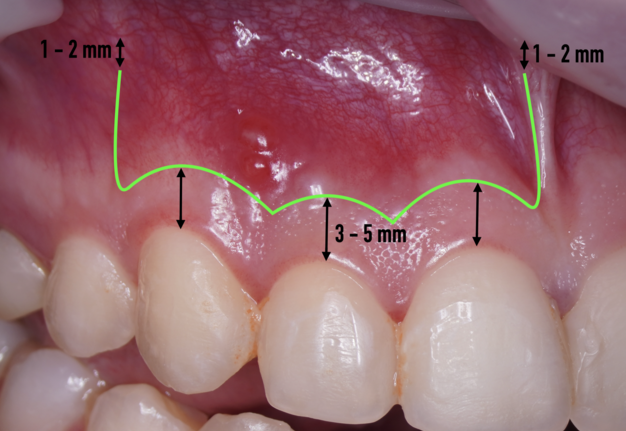
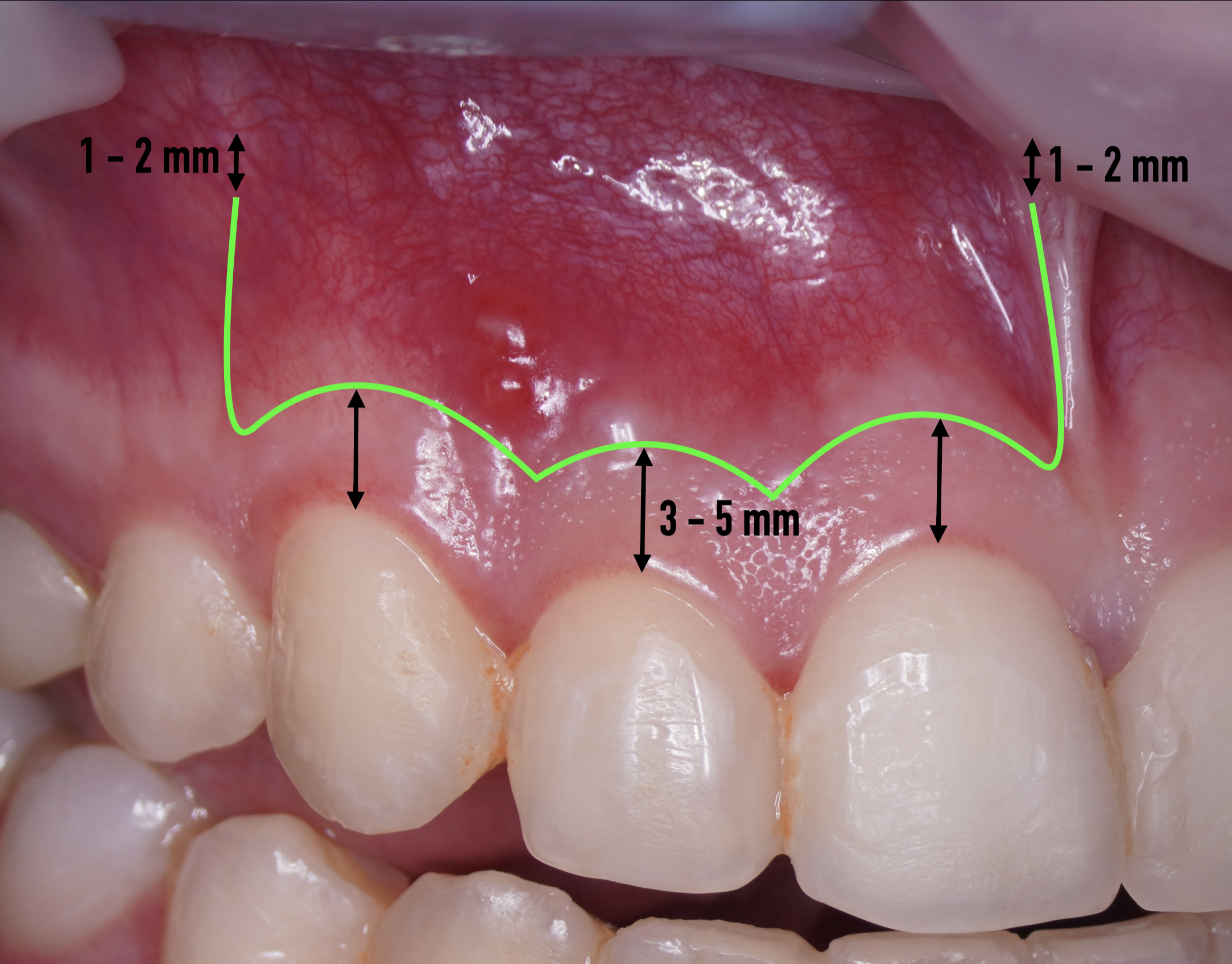
FIGURE 1. A schematic representation of a submarginal incision and flap.


FIGURE 2. An example of a submarginal incision and flap.
The submarginal flap is only to be used, when there is a broad zone of attached gingiva with a minimum of 2 mm [9]. The width of the attached gingiva is then calculated on the basis of the distance from the base of the sulcus to the linea girlandiformis (mucogingival junction) [6]. Consequently, the incision must be placed at least 2 mm from the depth of the gingival sulcus. Extensive periodontal probing should be done to establish the depth of the gingival sulcus before the incision is made [10]. Periodontal probing should be conducted not only around the causative tooth but also in the adjacent teeth.
According to Arnaldo Castellucci (2019) you also need to take into account the following features when performing the submarginal incision [5]:
-
The horizontal component is made about 1 mm coronal to the mucogingival junction.
-
The two terminal scallops, the mesial and the distal, should terminate horizontally, in order to make a 90° angle with the vertical releasing incision.
-
The incision must always involve one tooth mesial and one tooth distal to the one being operated on.
-
The two vertical incisions should be placed directly over healthy bone and should always avoid bony eminences.
-
The releasing incisions must be parallel and not divergent, so that the incision is rectangular and not trapezoidal. They must have a 90° rounded angle with the horizontal component and must be parallel to the long axis of the teeth, in order not to section the blood vessels that are also parallel to the long axis of the teeth.
-
Notably, the extent of the submarginal incision is influenced by multiple factors, including the clinician’s experience, the surgical site, cone beam computed tomography (CBCT) findings, and the overall clinical evaluation.
This flap design is recommended for maxillary anterior and posterior teeth in which reflection of marginal and interdental gingiva is contraindicated because of the presence of inflammation, particularly those that associated with fixed prostheses where esthetics are of great concern. The design is essentially limited to the maxilla. It is rarely amenable to the mandibular anterior teeth because it presents formidable wound closure problems in the thin, friable tissues of this region. And it is absolutely contraindicated in the mandibular posterior region because of anatomic considerations [11].
This flap is most indicated when there is an adequate amount of attached gingiva, the expected apical lesion or surgical bony access will not involve the incision margins, and there is no periodontal involvement in the surgical area, if the probing is within normal limits. It is also especially indicated in case of the presence of dental restorations in the frontal area, in order not to interfere with the cervical tissue and avoid later aesthetic problems [5]. However, where there are deep periodontal pockets, this type of incision is contraindicated, and a marginal incision should be performed instead [12].
Sometimes the frenulum of the upper lip is massive and for avoid its dissection, it is permissible to perform a submarginal flap with one vertical incision located more distally. It is worth recognizing that this approach is applied to a root with medium length on which microsurgery is performed (Figs 3 and 4).


FIGURE 3. A submarginal flap with one vertical incision located more distally.
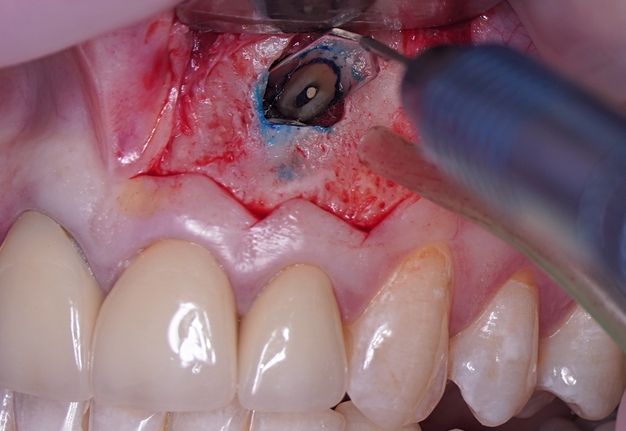
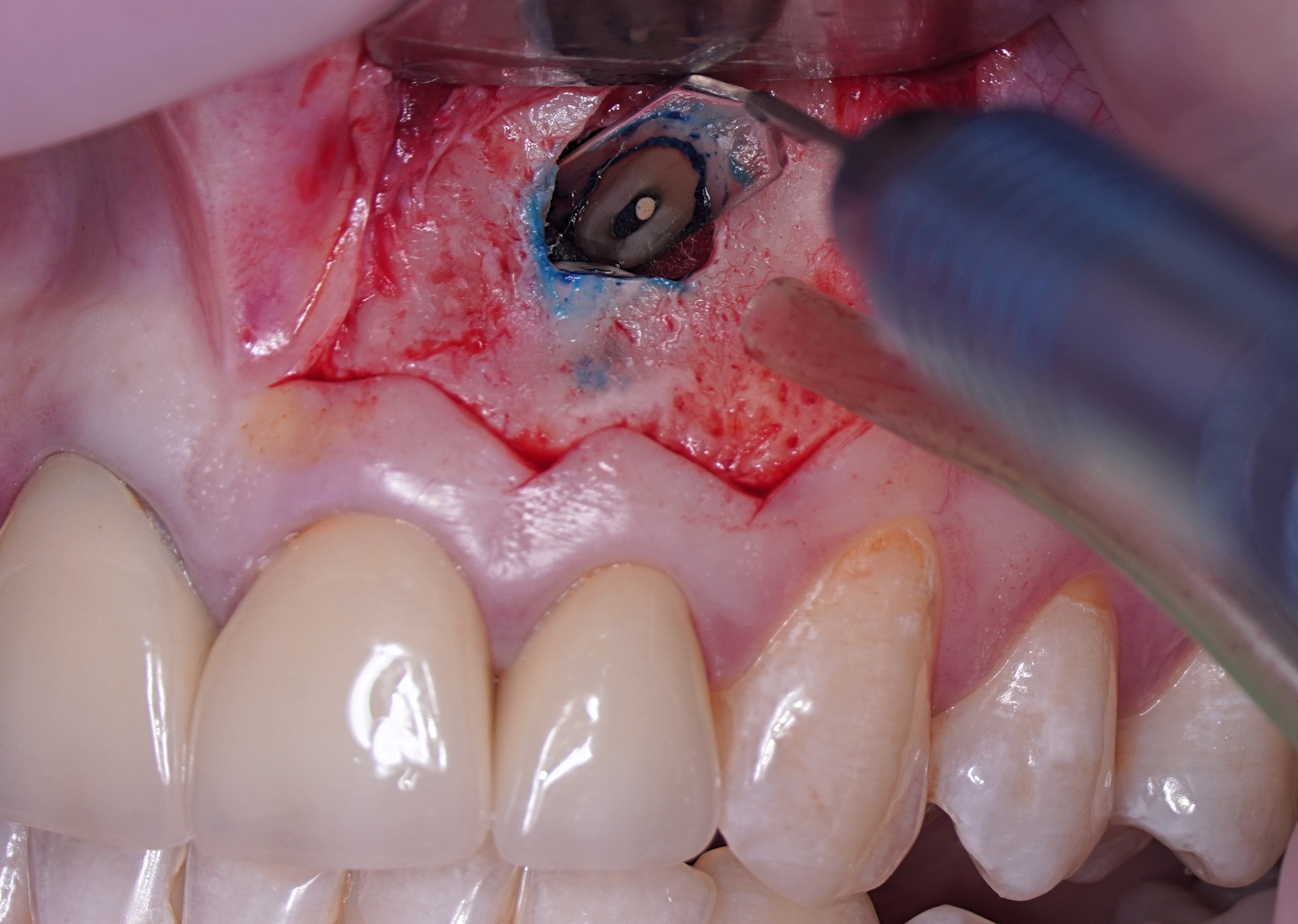
FIGURE 4. Another submarginal flap with one vertical incision located more distally shows good visibility of the resected root area.
According to Arens et al. (1998) the Ochsenbein-Luebke flap has the following advantages and disadvantages [8].
Advantages:
-
The flap is simple to incise and reflect.
-
The surgical site is readily visualized.
-
Access to the apex of the involved tooth is good.
-
The marginal gingiva is not disturbed, which greatly reduces the potential for gingival recession. This is particularly advantageous in the presence of prosthetic crowns.
-
Existing nonpathologic dehiscences are avoided because the gingival attachment is not disturbed.
-
Minimal effort is required to retract the flap.
-
Because the incision has good reference points, the flap is easily repositioned.
-
A patient is able to maintain good oral hygiene during the healing period.
Disadvantages:
-
Misjudging the size of the lesion may result in the incision(s) crossing the osseous defect.
-
Muscle attachments and frenums present anatomic obstructions that may require modification of the horizontal component.
-
If the horizontal incision is made too close to the free marginal gingiva, clefting may occur.
-
An unesthetic scar may form.
David Vreeland and Eddy Tidwell (1982) modified the submarginal incision by placing a scalloped horizontal incision 1 to 2 mm below the gingival margin [13]. An inverse-bevel incision splits the tissue until 1 to 2 mm below the crest of bone, from which point on a full thickness flap is reflected. After closure, the flap should cover the area of unreflected split thickness tissue. The authors claim that less exact replacement of the flap is required when using this approach. The type of incision described bears a high risk of postoperative necrosis, as the only blood supply to the unreflected marginal tissue is derived from the periodontal ligament [14, 15]. In addition, when 4/0 sutures are used, this critical area is further traumatized. Although the authors claim that scarring is “not much of a problem” the clinical pictures in the publication clearly demonstrate marked scar tissue formation, typical for submarginal incisions [16].
Once the apical microsurgery has been completed great care has to be taken in repositioning and suturing the elevated soft tissue. In fact, the ultimate esthetic result of the soft tissue manipulation depends on several factors such as the type of tissue, the type of incision, the choice of instruments used to incise, elevate, and retract the flap as well as careful reapproximation and a proper suture technique.
It is recommended to moisten the soft tissue with a wet gauze (sterile water or saline) before it is repositioned. The soft tissue can become dehydrated during the procedure and rehydrating it will return its natural elasticity and allows for easier reapproximation [17]. When flap shrinkage persists despite tissue rehydration, a supplementary horizontal incision may be performed at the flap base to generate a variable-thickness flap, thereby enhancing tissue adaptability and reducing contractile tension.
A good recommendation is compression of the repositioned flap with a saline-moistened piece of gauze is necessary to create a thin fibrin layer between flapped tissue and cortical bone [16].
Sutures are needed to hold the reapproximated flap in place and to allow healing of the wound by primary intention [18]. Accidental premature loss of sutures leads to delayed healing by secondary intention [19]. Bacterial colonization is an important factor leading to tissue reactions to intraoral sutures [20-24]. According to some authors [5, 10, 25, 26], monofilament synthetic sutures (polyamide, nylon) are the least traumatic, allow less bacterial migration, and are the materials of choice. The single knot, interrupted suture is used when a submarginal flap has been incised. The single knot suture has the advantage of being a stable, precise suture and allows for primary closure. On the other hand, it requires time and meticulous application, especially while suturing a submarginal flap in the anterior region [17]. Generally, 6-0 and 7-0 is used for suturing paramarginal incisions on attached gingiva. A surgeon knot is a modified square knot with two overhand knots, each completed in opposite directions. It is the most commonly used. Knots should be placed over tissue, never over an incision line [26] (Fig 5). When suturing is complete, chilled, sterile moist cotton gauze is again placed over the flap and pressure is applied for 5 minutes. Pressure to the area provides stability for the initial fibrin stage of clot formation and reduces the possibility of excessive postoperative bleeding and hematoma formation under the flap. The iced gauze also supports hemostasis. Final inspection of the area should confirm that all soft-tissue margins have been closely approximated, and bleeding has been controlled [10].


FIGURE 5. An example of sutures.
DISCUSSION
When choosing an incision, we need to consider not only the important factors listed above, but also possible risks and complications. The Ochsenbein-Luebke flap is typically associated with minimal gingival recession [7]. For example, von Arx et al. (2009) report significantly less recession for the submarginal incision compared with a sulcular and papilla base incision [27]. According to Kramper et al. (1984) the submarginal incision is the flap of choice in surgical endodontics, when not contraindicated by the anatomical location of the lesion (apicomarginal defects) or by insufficient attached gingival tissue [28].
One of the postulates of “The golden rules of the flap design” reads, “The incision must never cross a bone defect. Incisions should be made away from the lesion if possible” [29]. More recent research also supports this view “The underlying apical lesion or surgical bony access must not extend to the flap margins” [16]. Using CBCT, the surgeon can accurately measure the size of the bone defect and plan the incision design so that the incision is at a distance from the bone defect (or the area where the osteotomy will be performed). If the surgery is not planned carefully and the incision passes through a bone defect, the risk of complications associated with healing increases significantly. There is the risk of postoperative infection [12]. These complications are sometimes observed (Fig 6).


FIGURE 6. Healing complications associated with the incision passing through a bone defect (observation of Dr. Andrii Piholiev, Kharkiv, Ukraine).
Therefore, the selection of this type of incision requires thorough treatment planning [12]. To avoid the incision falling into an existing bone defect or a defect created by an osteotomy, it is rational to plan a submarginal incision. We can determine whether we can make it, according to the clinical situation of a patient by following approach. To do this, first we need to determine on the CBCT where the bone defect is located or where the osteotomy will take place. Then, using a virtual ruler, measure the distance from the incisal edge of the tooth on which the intervention will be performed to the beginning of the bone defect or osteotomy (Fig 7).

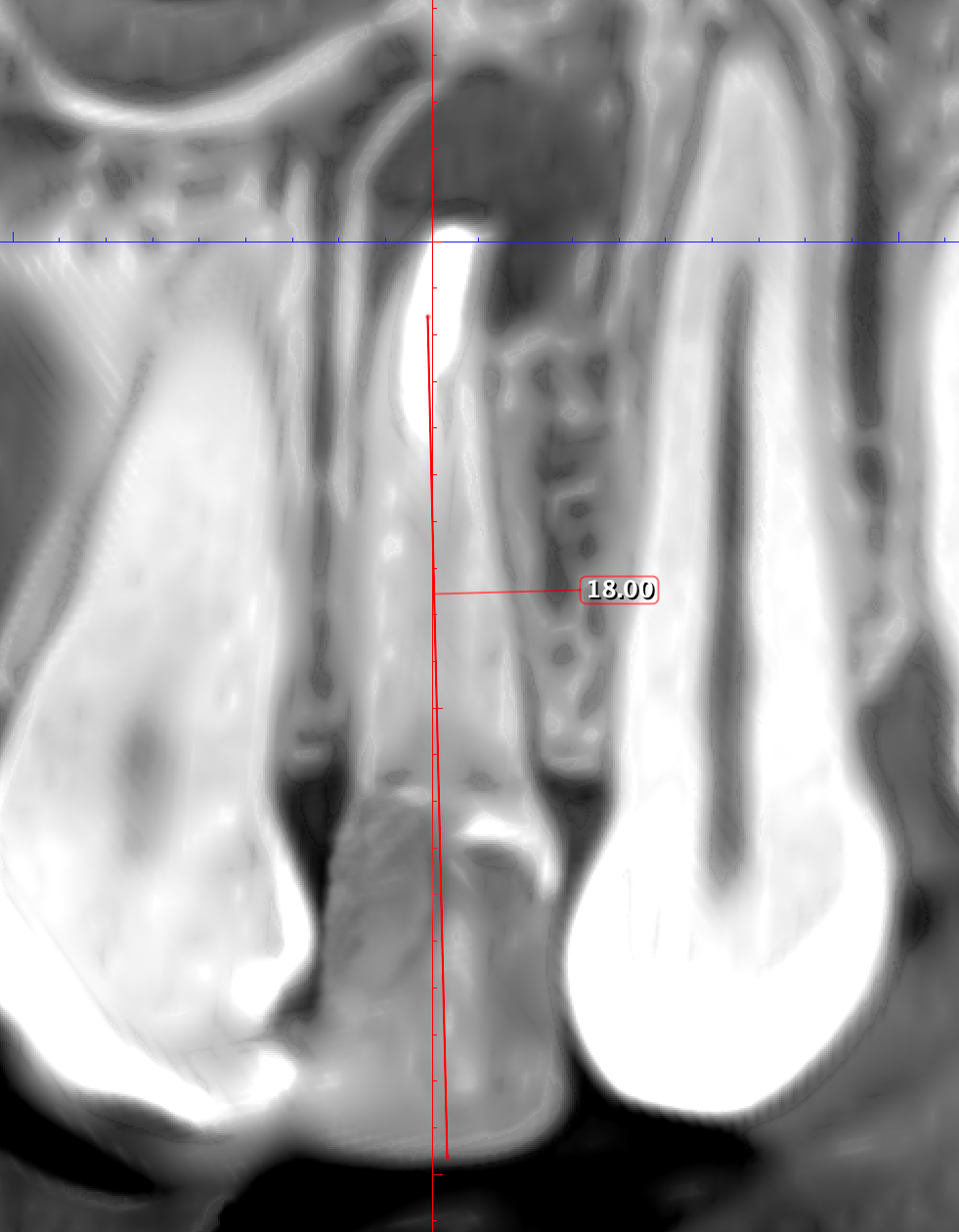
FIGURE 7. Preoperative CBCT of the tooth 22 (coronal plane).
We transfer this distance is transferred to a metal probe and fixed with an endodontic stopper. Next, we take a plastic probe and substitute it near the zenith of a tooth on which the intervention will be performed at a mark of 6 mm (3 mm must be retreated to perform a submarginal incision and another 3 mm is needed for the formed flap to overlap healthy bone tissue) (Fig 8).
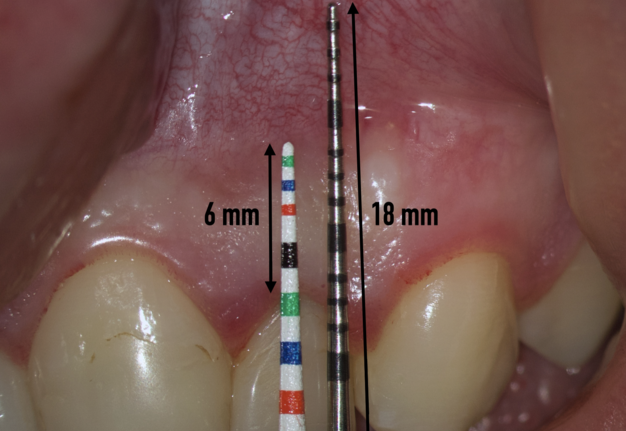
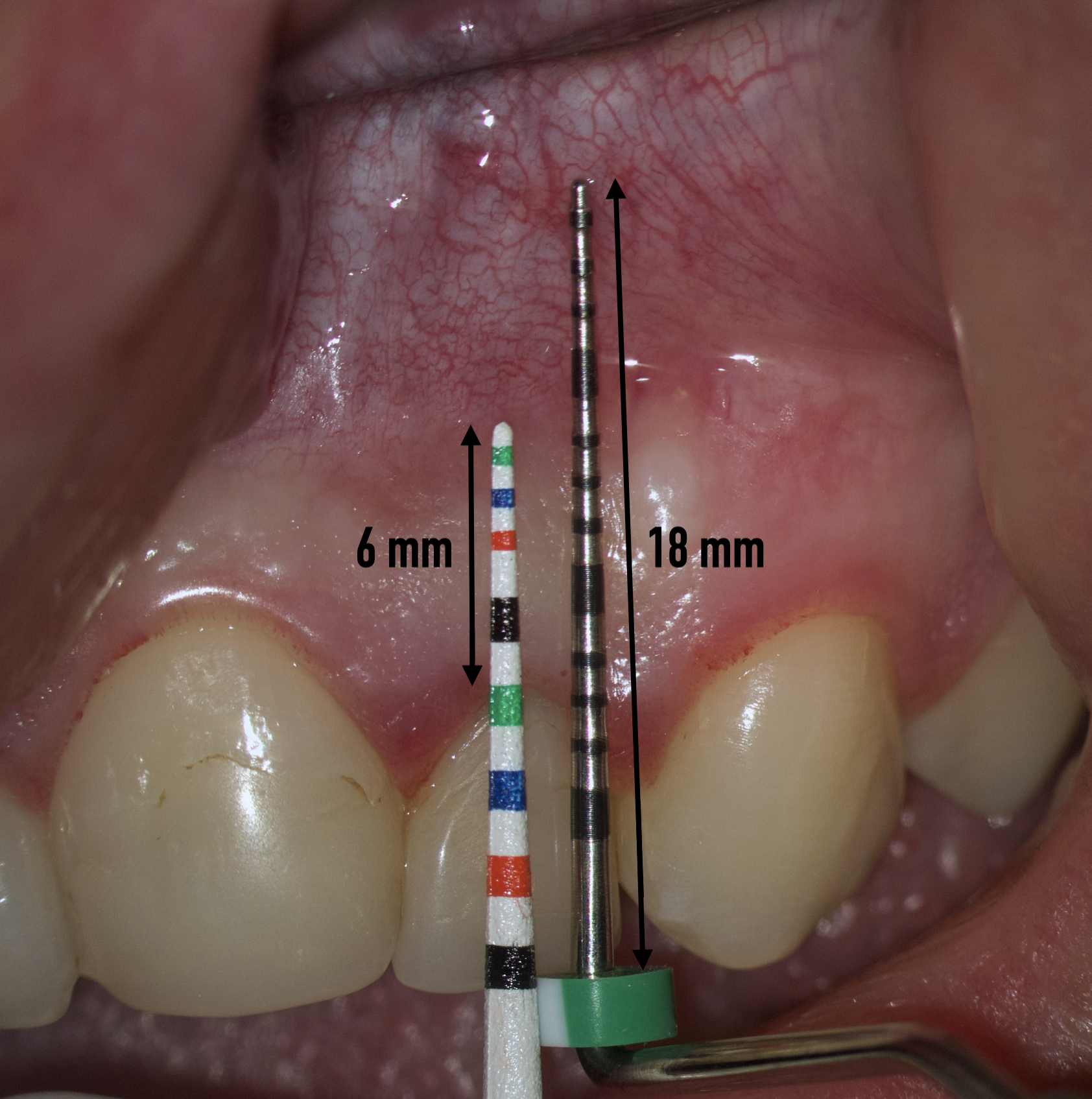
FIGURE 8. Transferring the planned lengths of the two probes to the vestibular surface.
We compare the lengths of the plastic and metal probes. The first option is when the metal probe is above the plastic one, then we can assure that the incision and the Ochsenbein-Luebke flap will accurately cover the bone defect and the submarginal incision is safe (Fig 9).
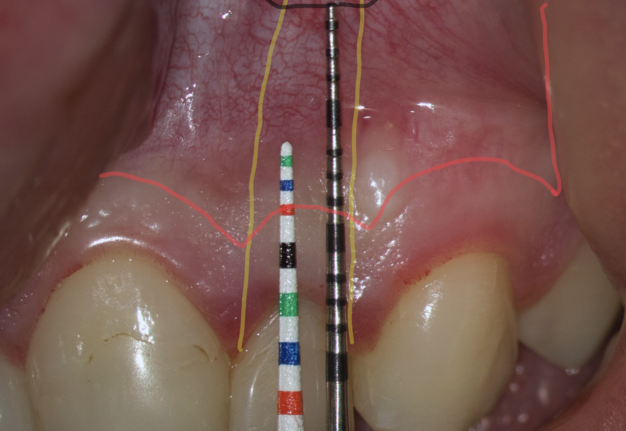
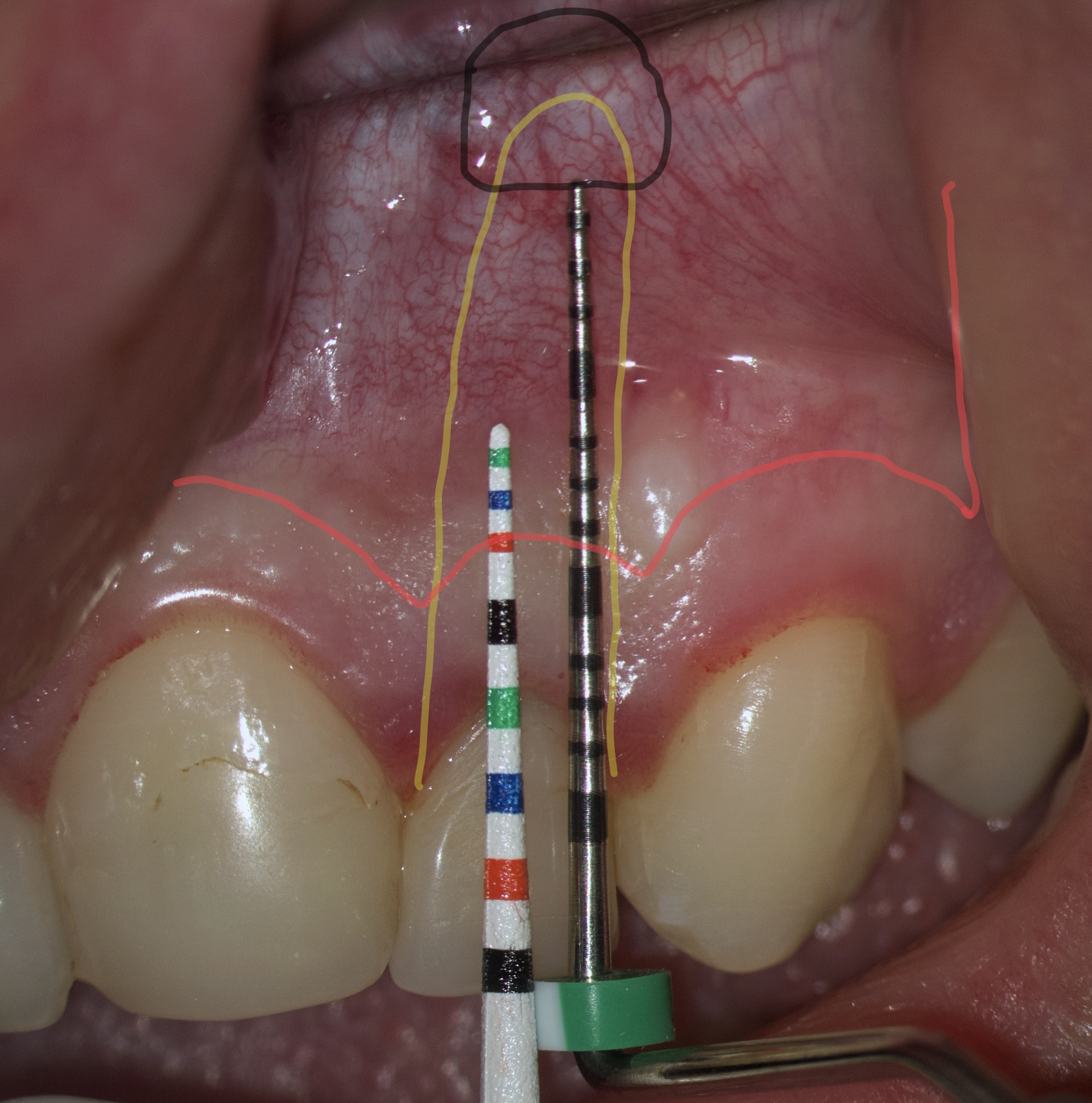
FIGURE 9. Comparison of the lengths of metal and plastic probes. The metal probe is above than the plastic one.
The second option is when the lengths of both probes are the same. This option is when a tooth has previously undergone root apex resection or a root is anatomically short or there is extensive periapical lesion. Under these conditions, we understand that there is still a safe distance of 3 mm so that the formed Ochsenbein-Luebke flap will also cover the bone defect and therefore, we can perform a submarginal incision and flap (Figs 10 and 11).


FIGURE 10. The lengths of both probes are the same.
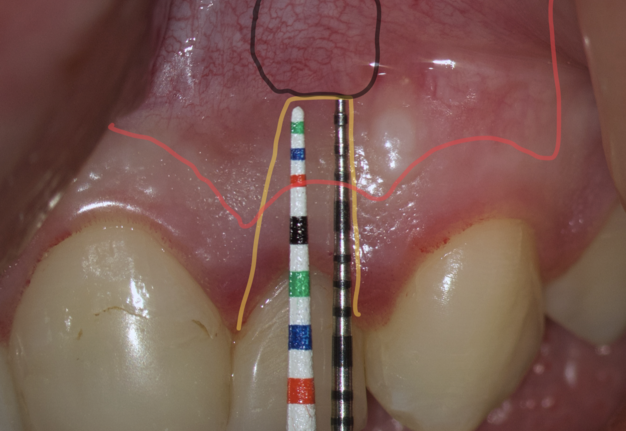
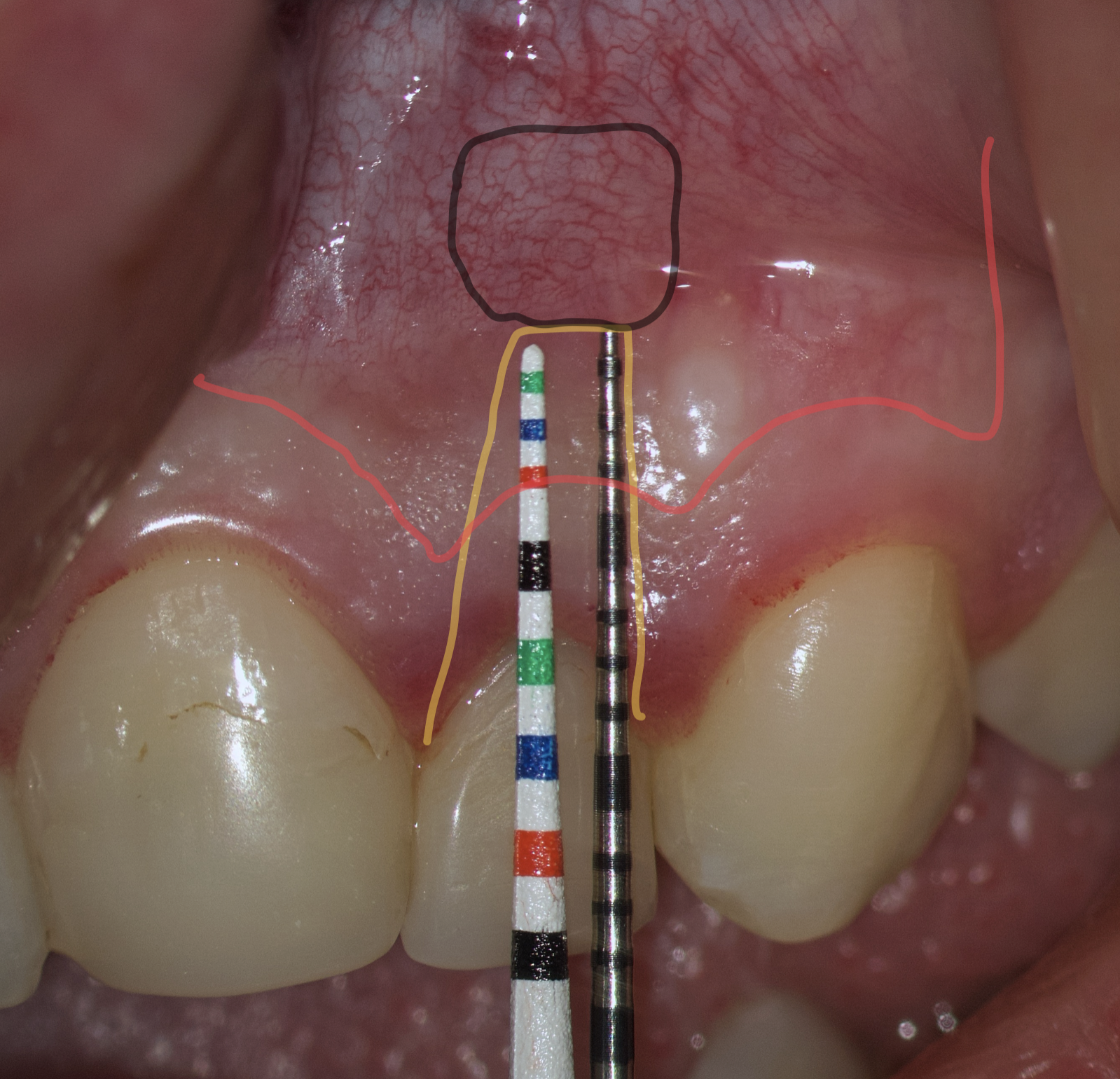
FIGURE 11. Schematic representation of the submarginal flap and the patient's clinical situation.
The third option is when the length of the metal probe is shorter than the plastic one. This option arises when the tooth has root resorption, root perforation or extensive periapical lesion extending to the alveolar crestal bone. In such conditions, performing a submarginal incision is contraindicated and it is preferable to use a papilla-base or intrasulcular incision (Figs 12 and 13).


FIGURE 12. The length of the metal probe is shorter than the plastic one.
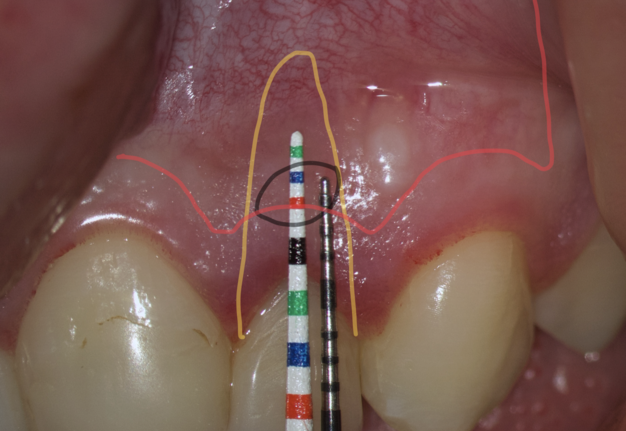
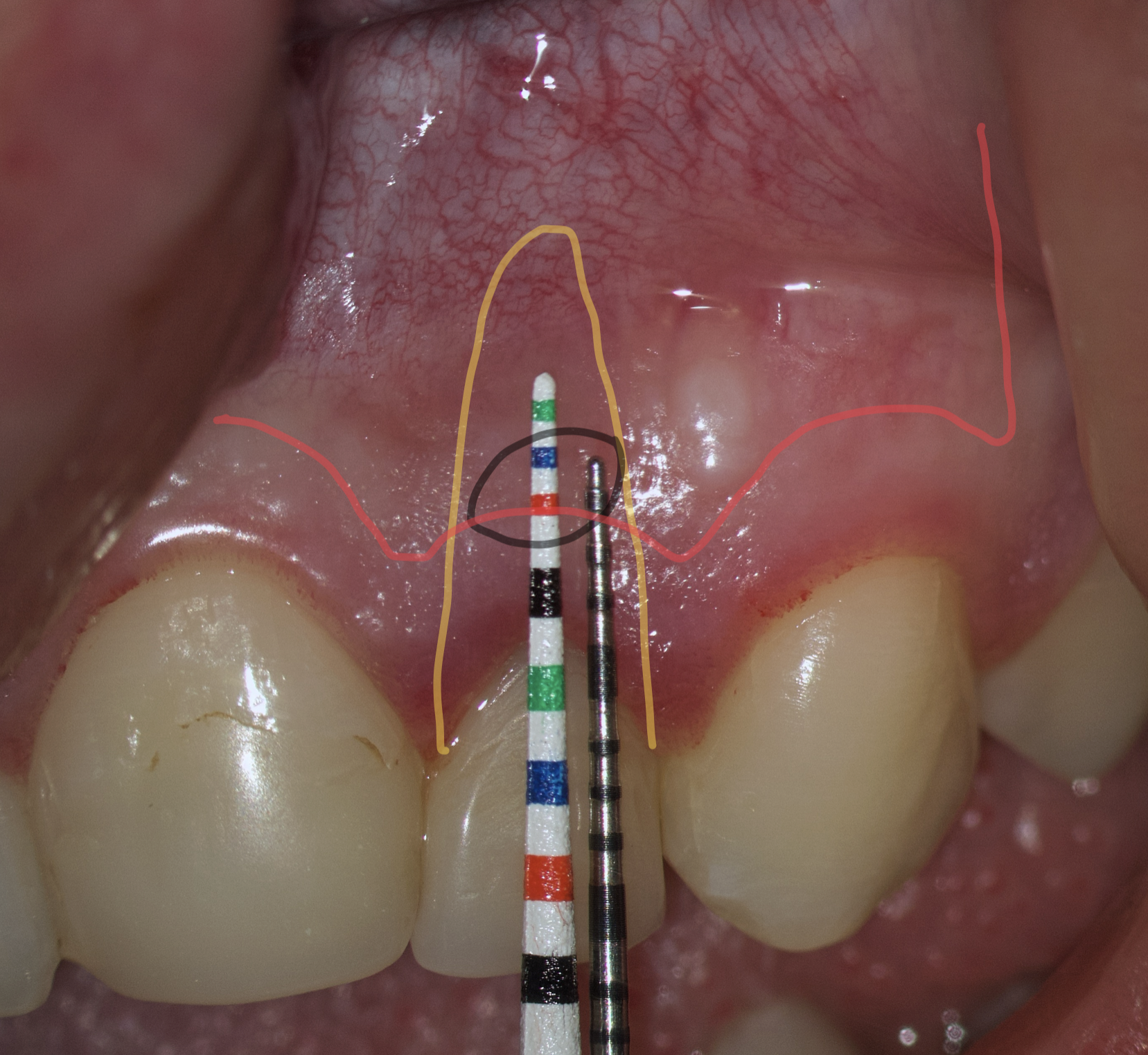
FIGURE 13. Schematic representation of the submarginal flap and the patient's clinical situation.
As a consequence of dehydration of the tissue, the Ochsenbein-Luebke flap sometimes tends to shrink during surgery resulting in tension and difficulty in replacing and securing it by suturing. Another disadvantage of the flap described in the literature is the risk of scarring (Fig 14) [7, 30].


FIGURE 14. Visible unaesthetic scar.
According to Lavagnoli and Carnevale (1984), the cause of the scar visible on the attached gingiva is the inclination of the blade to the underlying bone [30]. If the blade is used at 90° to the bone, the incision will involve the epithelium and the periosteum, and the two scars will be superimposed one on top of the other so that they become visible. On the other hand, according to the two authors, if the incision is beveled, the periosteal scar will be covered by healthy epithelium, which will hide the underlying scar. We know today that this is an old theory based on the fact that the periodontists use beveled incisions and they don’t have scars. However, we know today that scarring doesn’t depend on the inclination of the blade, but rather on the correct repositioning of the flap, the precise suturing done under the operating microscope and the early removal of the sutures, as will be described later. In conclusion, the blade can be used at 90° to the bone and by following the above suggestions, there is no risk of scarring [5].
One of the less well-described, rare and late complications of the Ochsenbein-Luebke incision is the occurrence of fenestrations in the soft tissues with baring bone. These fenestrations can be located both in the area of the attached gingiva, which corresponds to the horizontal component of the incision (Fig 15), and on the transition of attached gingiva into the alveolar mucosa, which corresponds to the vertical component of the incision (Fig 16).


FIGURE 15. Fenestration in the attached gingiva.


FIGURE 16. Fenestration in the transition of attached gingiva into the alveolar mucosa.
The development of soft tissue fenestrations with associated bone exposure is predominantly linked to a thin gingival biotype, suboptimal flap design, and inadequate wound closure.
CONCLUSION
When planning a microsurgical operation, many factors need to be evaluated to choose the most rational incision according to the clinical situation of a patient. Each incision has its own characteristics, indications, contraindications, advantages and disadvantages. The submarginal incision and flap are considered the most rational in an aesthetically important area. Taking into consideration clinical characteristics of a patient and accurate planning of the submarginal incision we minimize the risks and possible complications when performing endodontic microsurgery.
CONFLICT OF INTEREST
The author declares that he doesn’t have any conflict of interest.
REFERENCES (30)
- Newman MG, Carranza FA. Clinical periodontology and implantology. 14th ed. Elsevier. 2024, 1112 p.
- Gopikrishna, D. Kandaswamy, S. Nandini. Newer classification of endodontic flaps. Endodontology. 2005;17(2):14-19. https://doi.org/10.4103/0970-7212.347111
- Gutmann JL, Harrison JW. Surgical endodontics. St. Louis, Tokyo: Ishiyaku EuroAmerica, Inc. 1994; 468 p.
- Luebke RG. Surgical endodontics. Dent Clin North Am. 1974;18(2):379-391.
- Castellucci A. Microsurgical endodontics. Palm Beach Gardens: Edra Publishing. 2019. 312 p.
- Velvart P. Surgical endodontics. In: Bergenholtz G, Horsted-Bindslev P, Reit C, editors. Textbook of endodontology. 2nd ed. Oxford: Blackwell. 2003:348-365.
- Torabinejad M, Rubinstein R. The art and science of contemporary surgical endodontics. 1st ed. Quintessence Publishing. 2017; 336 p.
- Arens DE, Torabinejad M, Chivian N, Rubinstein R. Practical lessons in endodontic surgery. Quintessence Publishing. 1998; 224 p.
- Lang NP, Loe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol. 1972;43(10):623-627. https://doi.org/10.1902/jop.1972.43.10.623
- Berman L, Hargreaves K. Cohen’s pathways of the pulp. 12th ed. Elsevier. 2021; 928 p.
- Gutmann JL, Harrison JW. Posterior endodontic surgery: Anatomical considerations and clinical techniques. Int Endod J. 1985;18(1):8-34. https://doi.org/10.1111/j.1365-2591.1985.tb00415.x
- Bjørndal L, Kirkevang L-L, Whitworth J. Textbook of endodontology. 3rd ed. Wiley. 2018. 512 p.
- Vreeland DL, Tidwell E. Flap design for surgical endodontics. Oral Surg Oral Med Oral Pathol. 1982;54(4):461-465. https://doi.org/10.1016/0030-4220(82)90396-6
- Nobuto T, Yanagihara K, Teranishi Y, et al. Periosteal microvasculature in the dog alveolar process. J Periodontol. 1989;60(12):709-715. https://doi.org/10.1902/jop.1989.60.12.709
- Mörmann W, Ciancio SG. Blood supply of human gingiva following periodontal surgery. A fluorescein angiographic study. J Periodontol. 1977;48(11):681-692. https://doi.org/10.1902/jop.1977.48.11.681
- Velvart P, Peters C.I. Soft tissue management in endodontic surgery. J Endod. 2005;31(1):4-16. https://doi.org/10.1097/01.don.000014532.08454.5c
- Kim S, Kratchman S. Microsurgery in endodontics. 1st ed. Wiley-Blackwell. 2017; 256 p.
- Belcher JM. A perspective on periodontal microsurgery. Int J Periodontics Restorative Dent. 2001;21(2):191-196.
- Kon S, Caffesse RG, Castelli WA, Nasjleti CE. Revascularization following a combined gingival flap-split thickness flap procedure in monkeys. J Periodontol. 1984;55(6):345-351. https://doi.org/10.1902/jop.1984.55.6.345
- Lilly GE. Reaction of oral tissues to suture materials. Oral Surg Oral Med Oral Pathol. 1968;26(1):128-133. https://doi.org/10.1016/0030-4220(68)90232-6
- Lilly GE, Armstrong JH, Salem JE, Cutcher JL. Reaction of oral tissues to suture materials. 2. Oral Surg Oral Med Oral Pathol. 1968;26(4):592-599. https://doi.org/10.1016/0030-4220(68)90343-5
- Lilly GE, Salem JE, Armstrong JH, Cutcher JL. Reaction of oral tissues to suture materials. 3. Oral Surg Oral Med Oral Pathol. 1969;28(3):432-438. https://doi.org/10.1016/0030-4220(69)90239-4
- Lilly GE, Cutcher JL, Jones JC, Armstrong JH. Reaction of oral tissues to suture materials. 4. Oral Surg Oral Med Oral Pathol 1972;33(1):152-157. https://doi.org/10.1016/0030-4220(72)90221-6
- Lilly GE, Osbon DB, Hutchinson RA, Heflich RH. Clinical and bacteriologic aspects of polyglycolic acid sutures. J Oral Surg. 1973;31(2):103-105.
- Selvig KA, Biagiotti GR, Leknes KN, Wikesjo UM. Oral tissue reactions to suture materials. Int J Periodontics Restorative Dent. 1998;18(5):474-487.
- Merino E. Endodontic microsurgery. 1st ed. Quintessence Pub. 2009; 352 p.
- von Arx T, Salvi GE, Janner S, Jensen SS. Gingival recession following apical surgery in the esthetic zone: A clinical study with 70 cases. Eur J Esthetic Dent. 2009;4(1):28-45.
- Kramper B.J, Kaminski EJ, Osetec EM, Heuer MA. A comparative study of the wound healing of three types of flap design used in periapical surgery. J Endod. 1984;10(1):17-25.
- Arens DE, Adams WR, De Castro RA. Endodontic surgery. New York: Harper & Row.1984; p. 102-132.
- Lavagnoli G, Carnevale G. Tecniche chirurgiche in endodonzia: note tecnicocliniche sulla incisione della mucosa e sulla sutura. Dental Cadmos. 1984:13. (In Italian).